Angular Limb Deformity
November 18, 2024 · Dogs

SIGNALMENT: Cassidy, 10-month-old, female spayed, Bernese Mountain Dog Mix
INITIAL CONSULTATION:
Referral from another surgical specialty center
Since adoption 6 months prior (age of 4 months old), Cassidy had a progressive right pelvic limb lameness. Otherwise, Cassidy was systemically in good health.
Relevant Physical Examination Findings:
Ambulatory x 3 with a right pelvic limb non weight-bearing lameness
Right stifle – significantly decreased extension, normal flexion, stable varus/valgus stress, moderate effusion, grade IV/IV lateral patella luxation (LPL), stable femorotibial joint (no overt cranial drawer or tibial thrust), no crepitus, no audible ‘click’, no pivot shift, mild periarticular fibrosis (medial buttress)
Left stifle – nonpainful hyperextension, normal flexion, stable varus/valgus stress, no effusion, stable femoropatellar joint (no patella luxation), stable femorotibial joint (no cranial drawer or tibial thrust), no crepitus, no audible ‘click’, no pivot shift, no periarticular fibrosis (medial buttress)
Right quadriceps and hamstrings – moderate atrophy, normal tone
Left quadriceps and hamstrings – normal mass and tone
Diagnostics:
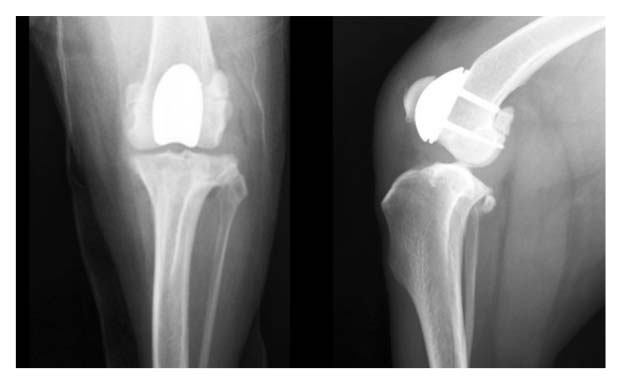
Due to the severe grade 4 right LPL, radiographs were made to assess for an underlying angular limb deformity, which was confirmed.

Further radiographs were not pursued due to the multiplanar (frontal, sagittal, and transverse) limb deformities, as deformities of this significant nature cannot be accurately assessed radiographically using a traditional segmental technique.
Accurate surgical planning for such severe deformities benefit from additional diagnostics, such as cross-sectional imaging, which was recommended and performed.
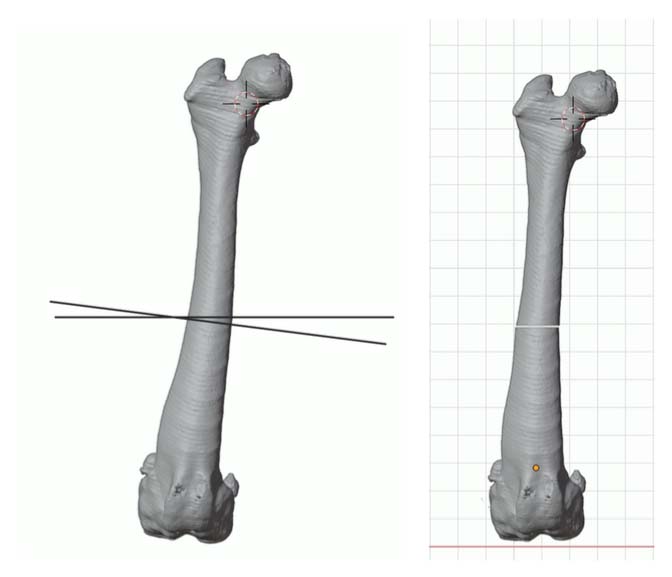
Pelvic limb computed tomography (CT) scan for computer-aided design (CAD)-based surgical planning was performed readily with sedation.
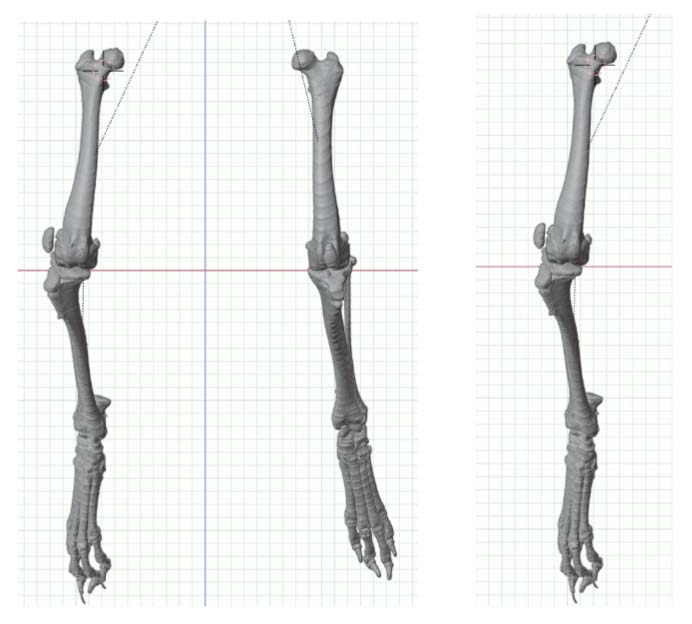
A method of planning and correction, commonly used in human surgery, has been adapted for the small-animal patient. This method is called the center of rotation of angulation (CORA). With this method, bone axes and joint orientation angles were made to provide guidance for accurate correction of angular limb deformities based on one standard set of geometric principles as they apply to osteotomies, regardless of the bone in question or the type of fixation device.
Final Diagnosis:
Right lateral patella luxation (LPL) – grade IV/IV
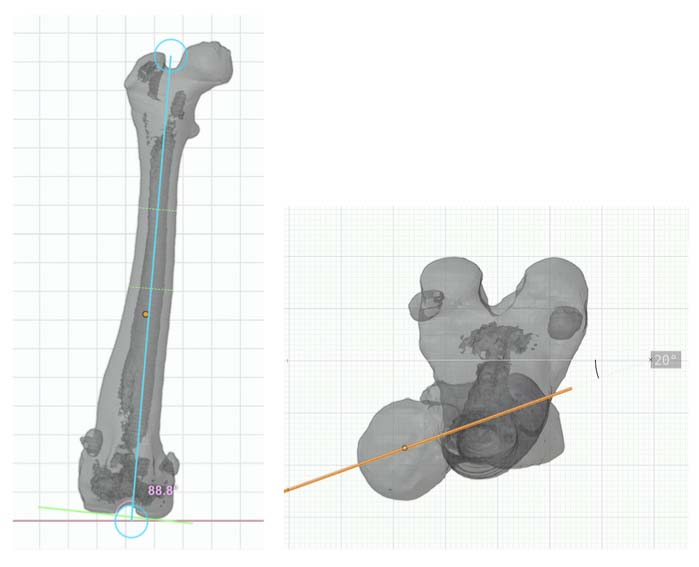
CT CAD-based approach to deformity planning documented two right femoral deformities:
Excessive anatomical lateral distal femoral angle (aLDFA) = 88.8 degrees
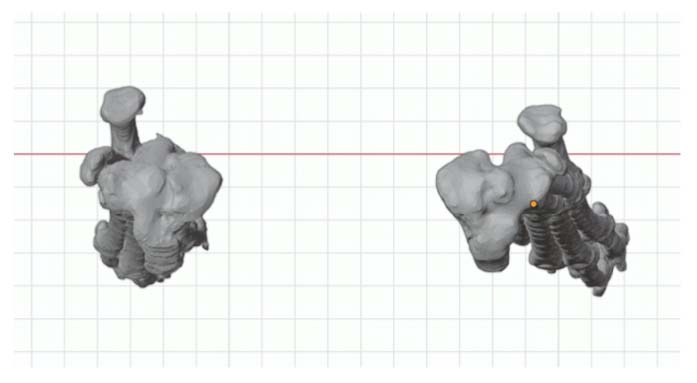
Femoral version 20 degrees
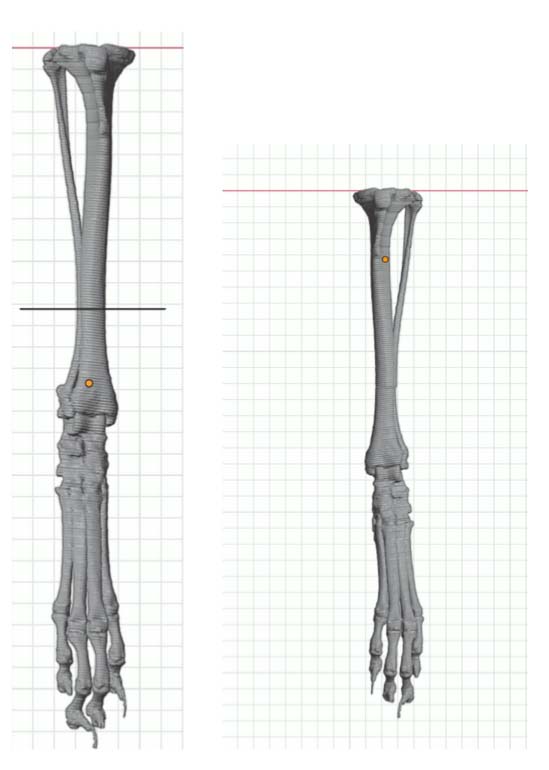
One right tibial deformity (19 degrees of excessive tibial internal torsion)
Surgical correction of the angular limb deformities was recommended, in order to successfully resolve the grade 4 patella luxation and provide proper joint alignment and joint loading, thus allowing for a functional and nonpainful limb.
Surgical Plan:
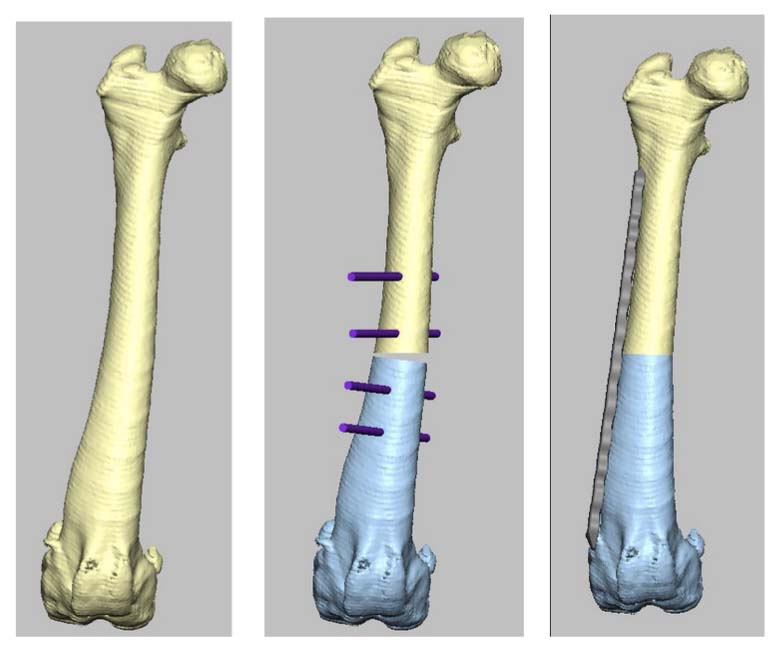
Correct the right femur angular limb deformities with a mid-diaphyseal oblique closing-wedge ostectomy centered at the CORA of the femoral deformity, which is located within the mid-diaphyseal (do not recommend a traditional distal femoral ostectomy (DFO) as this would result in a significant lateral femoral translation in this specific case). The trochlea is arthritic and hypoplastic, but not overtly deformed. In this case, a traditional block or wedge trochleoplasty is recommended rather than a patellar groove replacement (PGR). In addition, a corrective de-torsional tibial osteotomy has been recommended, as a tibial tuberosity transposition (TTT) is unlikely able to compensate for a torsion of this magnitude.
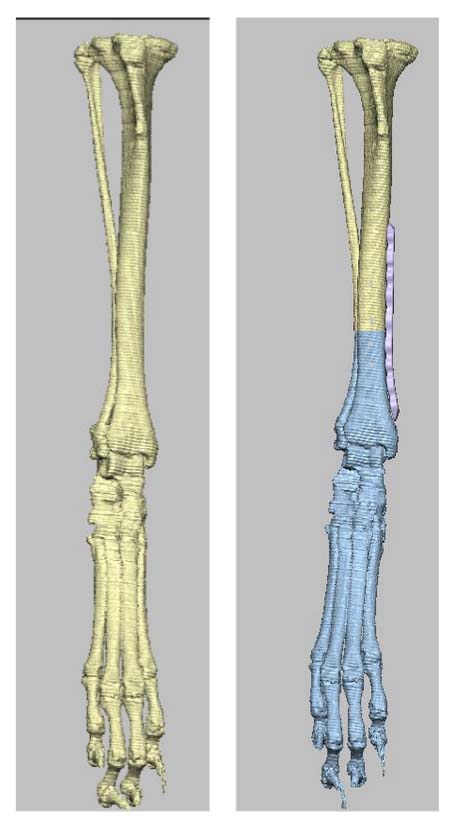
CT CAD-based surgical plan.
Surgical Procedures (7/17/24):
Right femoral mid-diaphysis bi-planar de-torsional medially based closing wedge ostectomy and internal fixation (lateral contoured locking straight plate and screws (Ti))
Right tibia distal diaphysis de-torsional osteotomy and internal fixation (medial contoured locking straight plate and screws (Ti))
Right femoral trochlear block recession
Right stifle lateral fasciotomy and joint capsulotomy
Right stifle medial retinacular and joint imbrication
Right tibial tuberosity transposition and internal fixation (cranio-caudal smooth Steinmann pin x 2)
Immediate Postoperative Recommendations:
No off leash, running, or jumping
Short and slow leash walks 4x daily for elimination purposes
Passive range of motion physical therapy in order to promote stifle range of motion due to chronicity of quadriceps contraction secondary to initial limb deformity, patella luxation, and non weight-bearing with stifle flexion.
Two Weeks Postoperative Update/Recommendations:
Skin incisions healed
Continue patella reduction
Stable femur and tibia
Improved limb usage (from non weight-bearing for 6 months preoperative to weight-bearing severe lameness)
Intense professional physical therapy, including underwater treadmill and passive range of motion, thus promoting continued weight-bearing, joint health, quadriceps stretching, and muscle mass. During these sessions, a muscle relaxant and nonsteroidal anti-inflammatory was prescribed.
Slow and controlled leash walking for 15-miutes, 4x daily. In addition, swimming/underwater treadmill encouraged.
Continued no off leash, running, or jumping.
Two Months Postoperative Update/Recommendations (9/10/24):
Owner reports that Cassidy is doing great and weight-bearing comfortably and consistently on the surgical leg.
Medications being administered only on physical therapy days (twice weekly): gabapentin, carprofen, and trazadone
Ambulatory x 4 with a right pelvic limb weight-bearing mild lameness (from non weight-bearing for 6 months preoperative to weight-bearing mild lameness)
Right stifle – no patellar ligament inflammation, no bruising, stable, no tibial thrust, nonpainful flexion/extension, full and restored complete range of flexion and extension, no pivot shift, no patellar luxation with normal tracking within femoral trochlear grove, lateral parapatellar and medial tibial skin incisions healed
Radiographs:


Osteotomies healed with stable implants, reduced patella, and joint alignment
Restored right stifle full range of motion and pain-free weight bearing on her right pelvic limb
Resolved grade 4 lateral patella luxation and angular limb deformities
Gradually resume normal activity over the following two weeks:
Week One: Allow unlimited walking, swimming, and bathing.
Week Two: Allow unlimited running, jumping, and playing for 10-15 minutes, then double the time each day until no time limit is achieved.
THREE and a HALF MONTHS POSTOPERATIVE UPDATE (10/31/24):
Owner updates: Cassidy is doing extremely well with no signs of lameness, stiffness, or discomfort. She has completed her physical therapy and runs, romps, and plays like crazy. In addition, she is off all medications and only takes a daily joint supplement.
With dedicated owners and physical therapists, Cassidy has restored a completely normal and nonpainful stifle joint range of motion with no lameness. In addition, no medications, restrictions, or additional treatments are required thus far.
Cassidy, from non weight-bearing for 6 months preoperative, to 3.5 months postoperative nonpainful limb usage and comfort.
Although not required for Cassidy, a patellar groove replacement (PGR) would be another option for those cases with significantly malformed femoral trochlear grooves and/or progressive femoropatellar degenerative joint disease later in life.